Symptom Comparison Tool: Akathisia vs. RLS
Disclaimer: This tool is for educational purposes only and is not a medical diagnosis. Always consult a healthcare provider before changing or stopping medications.
Analysis Results
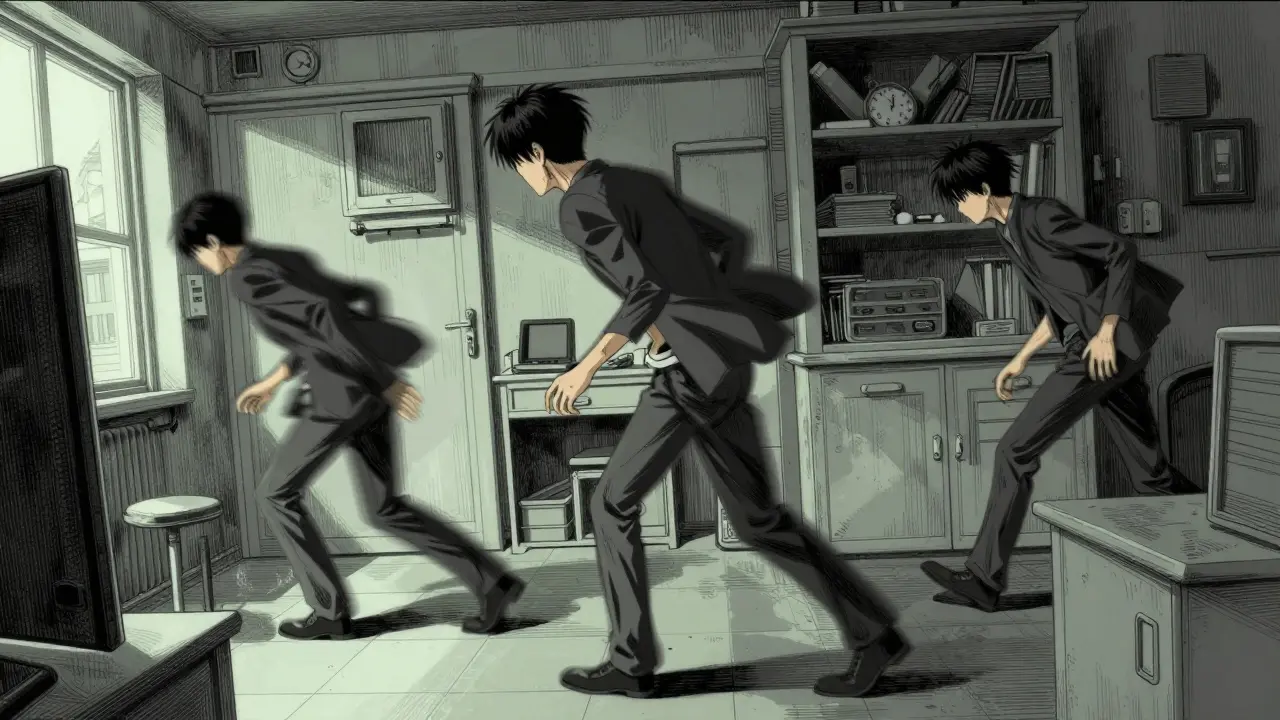
Understanding the difference between Akathisia is a medication-induced movement disorder characterized by a subjective feeling of inner restlessness and a compelling need to be in constant motion. It is primarily classified as an extrapyramidal side effect, meaning it affects the basal ganglia in the brain. and other similar sensations is critical for anyone taking psychiatric medications.
The Different Faces of Akathisia
Akathisia isn't a one-size-fits-all experience. Depending on when it starts and how long it lasts, clinicians categorize it into four main types. Recognizing which one you're dealing with helps determine how to handle the treatment.
- Acute Akathisia: This is the most common form. It usually pops up within days or weeks of starting a new medication or increasing a dose. It typically lasts less than six months.
- Chronic Akathisia: This is the long-haul version, where the restlessness persists for more than six months.
- Tardive Akathisia: This is a "late-onset" version that can appear months or even years after you've been on a steady dose of medication.
- Withdrawal Akathisia: A paradoxical reaction that happens within six weeks after you reduce your dose or stop a medication entirely.
Akathisia vs. Restless Legs Syndrome: How to Tell Them Apart
On the surface, akathisia and Restless Legs Syndrome (RLS) look identical. Both involve a desperate urge to move the legs. However, the "why" and "when" are completely different. If you're trying to figure out which one you have, look at your patterns.
RLS usually hits hardest when you're lying down at night or sitting still for long periods. It often has a genetic component or is linked to iron deficiency. The relief is usually immediate once you move. Akathisia, on the other hand, is a whole-body experience. While the legs are often the most active, the internal turmoil is generalized. Crucially, akathisia is directly tied to the timing of your medication. If the restlessness started shortly after you began an antipsychotic, it's much more likely to be akathisia.
| Feature | Akathisia | Restless Legs Syndrome (RLS) |
|---|---|---|
| Primary Trigger | Medication (Antipsychotics/Antiemetics) | Inactivity, Nighttime, Genetics |
| Sensation | Inner turmoil, "jumping out of skin" | Creepy-crawly or aching in limbs |
| Scope | Generalized body agitation | Primarily legs and feet |
| Timing | Correlates with drug dose changes | Occurs during rest or sleep |
| Response to Dopamine | Can be worsened by dopaminergics | Usually improved by dopaminergics |
The Culprits: Which Medications Cause This?
The most frequent cause is Antipsychotic Medications, which are used to treat schizophrenia and bipolar disorder. These drugs work by blocking dopamine receptors (specifically D2 receptors) in the brain. When too many receptors are blocked, the movement control center goes haywire.
First-generation antipsychotics, like Haloperidol, have a very high risk because they bind so strongly to those receptors. Second-generation options (atypicals) are generally safer, but they can still cause it. For example, risperidone has a higher incidence rate than newer drugs like lumateperone, which shows significantly lower rates of akathisia in clinical trials.
It's not just psychiatric drugs, though. Certain nausea medications, specifically Metoclopramide, can trigger the same reaction because they also affect dopamine pathways. If you've recently started a medication for stomach issues and suddenly feel like you can't sit still, this could be the reason.
Spotting the Red Flags: Recognition Protocols
Because akathisia is so often misdiagnosed as anxiety, you have to be your own advocate. If you're talking to a doctor, don't just say you're "restless." Be specific about the motor patterns. Do you find yourself constantly crossing and uncrossing your legs? Are you shifting your weight from foot to foot even when you're trying to be still? Are you pacing the room during your appointment?
Clinicians often use the Barnes Akathisia Rating Scale (BARS) to make an objective assessment. This tool looks at two things: your subjective feeling of inner unrest and the observable movements the doctor sees. A key diagnostic question to ask yourself is: "Does this feel like an emotional anxiety, or does it feel like a physical need to move that is independent of my mood?" If it's the latter, you're likely dealing with a movement disorder.
How to Treat and Manage the Turmoil
The most effective way to stop akathisia is to address the cause. This usually means reducing the dose or switching the medication entirely. For instance, some patients have reported feeling "back to themselves" within just a few days of tapering off a high-potency antipsychotic.
However, stopping a psychiatric medication abruptly can be dangerous. Tapering must be done under strict medical supervision. If the medication is absolutely necessary for your stability, doctors may add "counter-medications" to soothe the nervous system:
- Beta-Blockers: Propranolol is often the first choice. It helps dampen the physical agitation without interfering with the psychiatric effects of the main drug.
- Benzodiazepines: Drugs like Clonazepam can be used for short-term relief, especially when the distress is severe.
- Anticholinergics: These are sometimes used to balance the chemical signals in the brain, though they are generally less effective for akathisia than they are for other movement side effects like tremors.
Newer treatments are also emerging. Some research into selective serotonin antagonists like pimavanserin shows promise in reducing akathisia without compromising the primary treatment's efficacy. There is even exploration into using transcranial magnetic stimulation (TMS) to calm the overactive circuits in the brain.
The Danger of Misdiagnosis
We cannot overstate how dangerous it is to mistake akathisia for anxiety. In a typical clinical error, a patient reports feeling "extremely agitated." The doctor, thinking the patient's psychosis or anxiety is worsening, increases the dose of the antipsychotic. This adds more fuel to the fire, intensifying the akathisia. This cycle can lead to a state of "inner torture" that some patients describe as worse than the original psychiatric condition they were treating.
This escalation is linked to a spike in suicidal ideation and aggression. When a person feels they cannot escape their own skin and their doctor is making it worse, the psychological breaking point happens quickly. Accurate recognition isn't just about comfort; it's about safety.
Can akathisia go away on its own?
Generally, no. If it is caused by a medication, it will typically persist as long as the medication is in your system at that specific dose. It usually only resolves once the causative agent is reduced, stopped, or managed with a secondary medication like a beta-blocker.
Is akathisia permanent?
In most cases, it is reversible. Acute akathisia often disappears shortly after a dose adjustment. However, there is a form called "tardive akathisia" that appears after long-term use; this version can be more persistent and may require more complex long-term management strategies.
What is the fastest way to get relief?
The fastest relief usually comes from removing the trigger medication, but this must be done safely. For those who cannot stop their medication, a low dose of propranolol or a benzodiazepine can often provide rapid relief of the physical distress.
Does caffeine make it worse?
Yes. While caffeine doesn't cause akathisia, it is a stimulant that can amplify the feeling of restlessness and agitation, making the symptoms feel more intense and harder to ignore.
How do I explain this to my doctor if they think it's just anxiety?
Use physical descriptions rather than emotional ones. Instead of saying "I feel anxious," say "I have an irresistible physical urge to move my legs," or "I feel a physical tension in my muscles that only goes away when I pace." Mention exactly when the feeling started in relation to your last dose change.
Next Steps for Patients and Caregivers
If you suspect you or a loved one is experiencing medication-induced restlessness, start a movement diary. Note the time of day, the dose of medication taken, and exactly what the movement feels like. This data is invaluable for a doctor to distinguish between a psychiatric symptom and a drug-induced side effect.
If you're a caregiver, watch for "pacing in place" or constant leg-crossing during conversations. These are the hallmark objective signs. Encourage the patient to describe the extrapyramidal symptoms specifically as "physical」 rather than "mental" restlessness to help the clinician move toward the correct diagnosis.

David Snyder
It's great that there's a clear way to explain this to doctors. Getting the right terminology can really change the course of treatment and help people feel better much faster.
Kenzie Evans
Obviously, anyone with a brain knows this. The whole thing is just basic pharmacology. It's honestly pathetic that we even have to write guides on how to tell a doctor that your legs are moving because of a drug.
Scott Lofquist
Actually, the BARS scale is way too subjective to be the gold standard 🙄. You can't just rely on a checklist when the biochemical imbalance is this complex. Most people just misinterpret their own nerves 🤡.
Billy Wood
SICK GUIDE!!! STAY VIGILANT!!!
Randy Ryder
The distinction between the D2 receptor antagonism and the resulting extrapyramidal symptoms is the crux of the issue here. I wonder if the incidence rates vary significantly based on the lipophilicity of the specific antipsychotic used, or if it's purely about the binding affinity in the nigrostriatal pathway. It's a fascinating intersection of neurology and pharmacology.
rupa das
beta blockers just mask it they dont fix the cause
Olivia Lo
There is a profound phenomenological tension when one's internal somatic experience is dismissed as mere anxiety. The ontological shift from "mental distress" to "neurological dysfunction" is not just a clinical change but a liberation of the self from a perceived psychiatric failure. We must acknowledge the iatrogenic harm caused by the recursive loop of dose escalation.
Princess Busaco
I find it absolutely laughable that people think a simple diary is going to fix a systemic failure in the medical industrial complex, and frankly, the suggestion that we should just "be our own advocates" is such a tired trope because it puts the burden of care on the victim of the side effect rather than the prescribing physician who should have known the pharmacodynamics of the drug in the first place, which is just typical of how these things are handled these days where the patient is treated like a lab rat in a maze of trial and error while their sanity is slipping away minute by minute because they can't even sit still to think about how miserable they are.
Brooke Mowat
This is such a wild ride of a feeling! It's like your soul is vibing too fast for your body to keep up, totally trippy but in a bad way. Just keep pushin thru and find that balance, ya'll got this!!
Milo Tolley
The sheer tragedy of iatrogenic akathisia is just... peak horror!!! Who even thinks that increasing the dosage is a good move when the patient is literally vibrating out of their skin??? Absolutely catastrophic!!!
Sam Dyer
Only in this country do we let doctors play pin the tail on the symptom 🙄. Absolute clown show. Get your facts straight and don't let some suit tell you it's just "nerves" when your legs are doing a jig :P
Ikram Khan
Oh man, this is so vital! I've seen people struggle so much with this and they didn't even have a word for it! 😱 It's like a nightmare you can't wake up from! Please, everyone, read the part about the movement diary! It's a game changer!!
Becca Suttmiller
I appreciate the tip about using physical descriptions. It seems like a practical way to ensure the doctor focuses on the motor symptoms rather than the emotional state.
Mark Dueben
For anyone feeling overwhelmed, just remember you're not alone in this. It's a tough spot to be in, but taking small steps like logging your symptoms can really help you get a better outcome with your healthcare provider.