Polypharmacy Risk Checker
Identify Dangerous Medication Combinations
This tool helps you check your medication combinations for potential interactions based on the Beers Criteria and clinical evidence. Enter your medications to see if any dangerous combinations exist.
Important: This tool is for informational purposes only. Always consult your healthcare provider or pharmacist for medical advice.
Results
More than 1 in 3 adults over 60 in the U.S. are taking five or more prescription drugs every day. It’s not uncommon. But what’s dangerous is that most people don’t realize how many of these medications are working against each other. A simple combo - like blood pressure pills and a common cold remedy - can send someone to the ER. The polypharmacy risk isn’t just about taking too many pills. It’s about which ones you’re taking together.
What Exactly Is Polypharmacy?
Polypharmacy isn’t a diagnosis. It’s a red flag. The medical definition is simple: taking five or more medications at the same time. But that number doesn’t tell the whole story. Two people could both be on five drugs, but one is at high risk while the other isn’t. It all depends on the types of drugs and how they interact.
According to the CDC, 20% of adults between 40 and 70 take five or more prescriptions. That number jumps to over 33% for those in their 60s and 70s. And it’s not just prescriptions. Over-the-counter painkillers, herbal supplements, and even vitamins can be part of the problem. One study found that 40% of dangerous drug interactions in cancer patients came from non-prescription items.
Here’s the hard truth: each new medication you add increases your chance of a major drug interaction by nearly 40%. That’s not a small risk. It’s a snowball effect. One drug causes dizziness, so you get another to fix it - only that second drug makes the dizziness worse. This is called a prescribing cascade. And it’s happening more often than you think.
The Most Dangerous Medication Combos
Not all drug combinations are equal. Some are quietly dangerous. Others are ticking time bombs. Here are the top offenders backed by real clinical data:
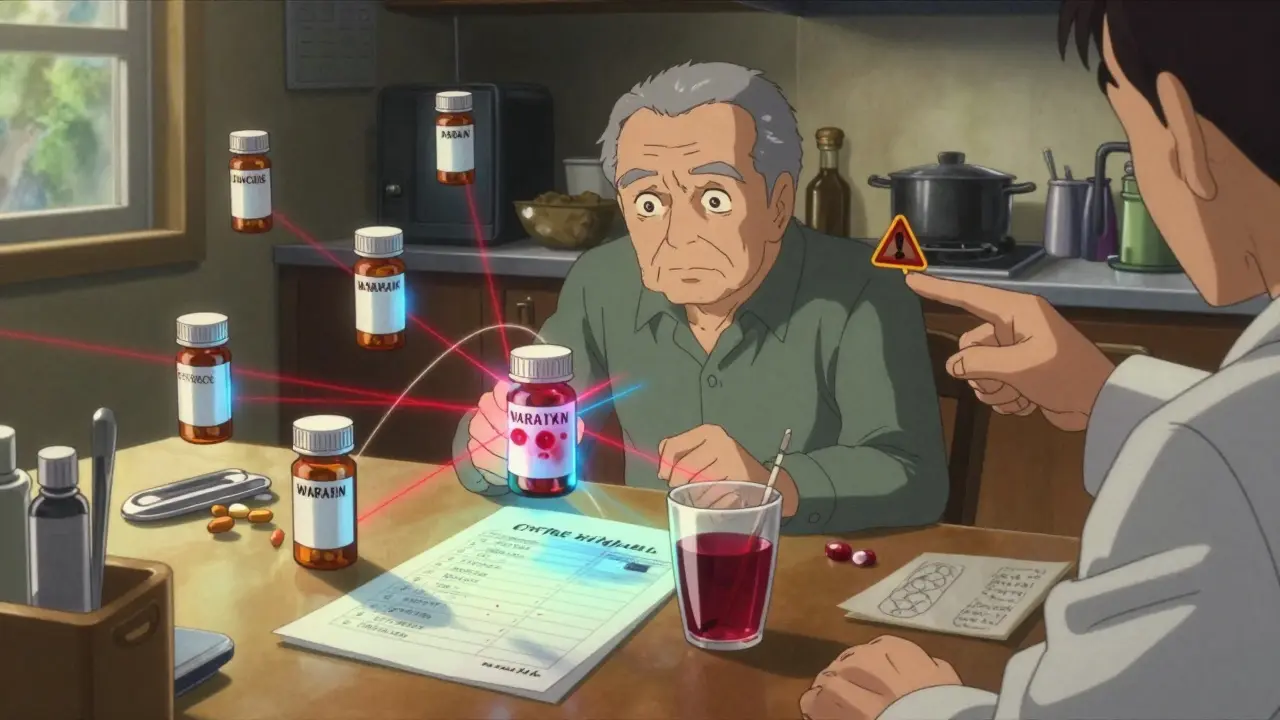
- Warfarin + Cranberry Juice: Warfarin (Coumadin) is a blood thinner. Cranberry juice blocks how your body breaks it down. Result? Your blood can’t clot at all. One glass a day can send you to the hospital with internal bleeding.
- Statins + Grapefruit Juice: If you’re on simvastatin or atorvastatin, grapefruit juice can cause your muscle cells to break down. This is rhabdomyolysis - a life-threatening condition that can lead to kidney failure.
- Blood Pressure Meds + Decongestants: Sudafed and similar OTC cold meds can spike your blood pressure. For someone already on lisinopril or metoprolol, this combo can trigger a stroke or heart attack.
- Acetaminophen + Oxycodone + Prochlorperazine: This trio shows up again and again in ER visits. The painkiller and nausea med both cause drowsiness. Add acetaminophen (often in the same pill as oxycodone), and your liver is under double pressure. The result? Severe dizziness, confusion, falls.
- Benzodiazepines + Opioids: This combo is on the Beers Criteria list for a reason. Both depress breathing. In older adults, this combination increases the risk of fatal overdose by 300%.
And it’s not just these five. A 2022 study of 718 cancer patients found that lisinopril, furosemide, and calcium supplements were involved in the most drug interactions. Why? Because they’re common. Everyone gets them. But nobody tells you how they play with other drugs.
The Beers Criteria: Your First Line of Defense
The American Geriatrics Society updated the Beers Criteria in 2019 - and it’s the most trusted tool doctors use to spot risky prescriptions in older adults. It’s not a guess. It’s evidence-based. Here’s what it flags:
- Strong anticholinergics like diphenhydramine (Benadryl), oxybutynin, and tricyclic antidepressants. These cause brain fog, constipation, urinary retention, and increase dementia risk.
- Benzodiazepines like lorazepam (Ativan) and diazepam (Valium). They’re sedating. They’re addictive. And they’re far too often prescribed for sleep or anxiety in seniors.
- Alpha-blockers like doxazosin and terazosin. Used for prostate issues, they cause dangerous drops in blood pressure when standing up - leading to falls.
- NSAIDs like ibuprofen and naproxen. They’re okay for occasional use. But daily use with blood pressure meds? That’s a recipe for kidney damage.
If you’re on any of these - especially two or more - you’re at higher risk. The Beers Criteria isn’t about stopping meds. It’s about asking: Is this still necessary?
How to Build Your Own Polypharmacy Risk Checklist
You don’t need a doctor to start. You need a pen, a list, and 30 minutes. Here’s how to build your own checklist:
- Make a complete list. Write down every pill, patch, liquid, and supplement. Include vitamins, herbal teas, and OTC drugs. Don’t forget the ones you only take “as needed.”
- Check for red flags. Use the Beers Criteria list above. Cross out anything that matches. If you’re unsure, look up the drug name + “Beers Criteria” online.
- Spot the dangerous combos. Look for the high-risk pairings we listed. If you’re on warfarin and drink grapefruit juice? That’s a red flag. If you take Benadryl for sleep and also take a bladder med? Double red flag.
- Ask about purpose. For each drug, ask: Why am I taking this? If the answer is “I’ve always taken it” or “My doctor said so,” that’s not enough. Every medication should have a clear reason.
- Find the cascade. Are you taking a laxative because of opioid constipation? Are you on a diuretic because your blood pressure meds made you swell? These are signs of a prescribing cascade. Each new drug is covering up a side effect from the last.
Keep this list with you. Bring it to every appointment. Even if you see a new specialist, give them this list. They don’t know your full history unless you give it to them.
Pharmacists Are Your Secret Weapon
Most people think pharmacists just fill prescriptions. They’re wrong. Pharmacists are trained to spot interactions before they happen. They know how grapefruit affects statins. They know why you shouldn’t mix melatonin with blood thinners. And they’re often more up-to-date than your doctor.
Ask your pharmacist for a free medication review. Bring your full list. Ask: “Are any of these drugs working against each other?” Most pharmacies offer this service - no appointment needed. One study found that pharmacist-led reviews reduced dangerous interactions by 65% in older adults.
Don’t wait for a problem. Go before you have one.
Deprescribing: Less Is Sometimes More
It’s not always about adding more drugs. Sometimes, the best treatment is stopping one.
Deprescribing means carefully removing medications that aren’t helping - or are hurting. It’s not quitting cold turkey. It’s a slow, monitored plan. The American Academy of Family Physicians recommends this step-by-step approach:
- Identify medications with no clear purpose
- Check for interactions using tools like the Beers Criteria
- Start with the lowest-risk drug to stop
- Reduce the dose slowly
- Monitor symptoms closely
- Reassess every few weeks
One 72-year-old cancer patient reduced her meds from 12 to 7 using the ARMOR method (Assess, Review, Minimize, Optimize, Reassess). She stopped feeling dizzy. Her energy came back. And her monthly drug bill dropped by $400.
What Happens If You Do Nothing?
Every year, 1.3 million older adults go to the ER because of bad drug reactions. 350,000 of them end up hospitalized. And 27.8% of all hospital admissions for people over 65 are caused by medications.
It’s not just about emergencies. The quiet dangers are worse. Falls from dizziness. Confusion that looks like dementia. Kidney damage from NSAIDs. Liver failure from too much acetaminophen. These aren’t rare. They’re predictable.
And the cost? Over $37 billion a year - just for medications. Add ER visits, hospital stays, and long-term care, and the real number is much higher.
There’s no magic pill. But there is a simple habit: review your meds every 3 to 6 months. Keep a list. Ask questions. Talk to your pharmacist. If you’re taking five or more drugs, you owe it to yourself to do this.
What’s Next?
The future of polypharmacy safety is coming. Tools are being built that use AI to predict interactions based on your genetics, your habits, and your real-time health data. Smart pill bottles that track when you take your meds. Wearables that detect early signs of dizziness or low blood pressure.
But those tools won’t help if you don’t start now. You don’t need a high-tech app to save your life. You need a list. A question. A conversation.
What is considered polypharmacy?
Polypharmacy is defined as taking five or more medications regularly, including prescription drugs, over-the-counter medicines, and supplements. It’s not just about the number - it’s about whether those drugs interact in harmful ways. The risk increases with each additional medication.
Which drug combinations are the most dangerous?
The most dangerous combinations include warfarin with cranberry juice (increases bleeding risk), statins with grapefruit juice (can cause muscle breakdown), blood pressure meds with decongestants (can trigger stroke), benzodiazepines with opioids (can stop breathing), and anticholinergics like Benadryl with other sedatives (worsens confusion and falls).
How can I check if my medications are interacting?
Start by making a complete list of everything you take - including vitamins and OTC drugs. Use the Beers Criteria to identify risky medications for older adults. Then, ask your pharmacist for a free medication review. They can spot interactions your doctor might miss.
Can I stop taking some of my meds on my own?
No. Never stop a medication without talking to your doctor or pharmacist. Some drugs need to be tapered slowly. Stopping suddenly can cause withdrawal, rebound high blood pressure, or seizures. Always work with a healthcare provider to safely reduce or remove unnecessary medications.
How often should I review my medications?
At least every 3 to 6 months - or after any new prescription, hospital stay, or change in health. If you’re taking five or more drugs, make this a regular habit. Keep your list updated and bring it to every appointment.

Aisling Maguire
Just did my med review today and holy cow-I had no idea cranberry juice and warfarin were a death combo. I drink that stuff daily for 'UTI prevention.' Guess I'm switching to water. Thanks for the wake-up call!
Sumit Mohan Saxena
The data presented is statistically significant and clinically validated. The Beers Criteria, as published by the American Geriatrics Society, remains the gold standard for identifying potentially inappropriate medication use in older adults. Pharmacist-led interventions have demonstrated a 62.7% reduction in adverse drug events in randomized controlled trials. It is imperative that patients maintain an updated medication list and seek formal medication reconciliation.
Brandon Vasquez
My mom’s on 8 meds. I made her a spreadsheet. Color-coded. Added expiration dates. She brings it to every appointment now. No more 'I think I take this once a day' moments. Simple. Free. Life-saving.
Vikas Meshram
You people are clueless. The pharmaceutical industry is pushing these drugs to make money. The FDA is corrupt. I stopped all my meds last year after reading a Reddit thread. My blood pressure is better. My energy is higher. They don't want you to know this. They profit from your dependency.
Ben Estella
So let me get this straight-Americans are dying because they’re too lazy to read labels? We got free pharmacies, free doctors, free apps. If you can’t handle 5 pills, maybe you shouldn’t be alive. This isn’t rocket science. It’s basic responsibility.
Jimmy Quilty
Did you know the CDC is funded by Big Pharma? That’s why they downplay the real dangers. I’ve been tracking my meds since 2018 and I’m convinced they’re poisoning us with microchips through the pills. The 'Beers Criteria' is just a distraction. Real change? It’s in the shadows. I’ve got receipts.
Miranda Anderson
I’ve been thinking about this a lot since my dad had that fall last year. He was on three meds that made him dizzy-two for blood pressure, one for sleep. He didn’t even realize they were connected. We sat down with his pharmacist and cut one out. He hasn’t stumbled since. It’s wild how something so simple can change everything. I wish more people knew this stuff.
Gigi Valdez
Pharmacists are underutilized. Their expertise in drug interactions is often overlooked in favor of physician-centric models. A systematic review published in JAMA Internal Medicine in 2021 confirmed that pharmacist-led medication reviews significantly reduce hospitalizations due to adverse drug events. This is not anecdotal-it is evidence-based practice.
Sneha Mahapatra
There’s a quiet wisdom in letting go. We’re taught to fix, to add, to control-but sometimes healing is in the subtraction. Each pill we take is a signal to the body: 'Something is wrong.' But what if the body is trying to heal itself, and we’re just drowning it in noise? I don’t know if I’ll ever stop all my meds… but I’m learning to ask why I take each one. That’s the first step toward peace.
bill cook
I’ve been on 11 meds for 12 years. I’m 71. I’m alive. So what’s the point of this? You think I’m gonna stop because some guy on the internet says so? I’ve been through chemo, two heart attacks, and a stroke. You don’t know my life. Don’t lecture me.
Byron Duvall
They say 'five or more meds' but they never mention that 80% of those are for symptoms caused by other meds. The system is broken. They sell you a pill for the side effect of the pill they sold you last month. It’s a pyramid scheme with heart pills.
Aisling Maguire
Wait-so you’re saying Benadryl makes you dizzy AND causes dementia? 😱 I’ve been taking it for sleep since college. I just thought I was getting old. I’m deleting it from my list tonight. Thanks for the reality check.